Guillain-Barre syndrome.
Overview
Guillain-Barre (gee-YAH-buh-RAY) syndrome is a rare disorder in which your body’s immune system attacks your nerves. Weakness and tingling in your hands and feet are usually the first symptoms.
These sensations can quickly spread, eventually paralyzing your whole body. In its most severe form, Guillain-Barre syndrome is a medical emergency. Most people with the condition must be hospitalized to receive treatment.
The exact cause of Guillain-Barre syndrome is unknown. However, two-thirds of patients report symptoms of an infection in the six weeks preceding. These include COVID-19, respiratory or gastrointestinal infection or Zika virus.
There’s no known cure for Guillain-Barre syndrome, but several treatments can ease symptoms and reduce the duration of the illness. Although most people recover completely from Guillain-Barre syndrome, some severe cases can be fatal. While recovery may take up to several years, most people can walk again six months after symptoms first start. Some people may have lasting effects from it, such as weakness, numbness or fatigue.
Symptoms
Guillain-Barre syndrome often begins with tingling and weakness starting in your feet and legs and spreading to your upper body and arms. Some people notice the first symptoms in the arms or face. As Guillain-Barre syndrome progresses, muscle weakness can turn into paralysis.
Signs and symptoms of Guillain-Barre syndrome may include:
- A pins and needles sensation in your fingers, toes, ankles or wrists
- Weakness in your legs that spreads to your upper body
- Unsteady walking or inability to walk or climb stairs
- Difficulty with facial movements, including speaking, chewing or swallowing
- Double vision or inability to move the eyes
- Severe pain that may feel achy, shooting or cramp-like and may be worse at night
- Difficulty with bladder control or bowel function
- Rapid heart rate
- Low or high blood pressure
- Difficulty breathing
People with Guillain-Barre syndrome usually experience their most significant weakness within two weeks after symptoms begin.
Types
Guillain-Barre syndrome has several forms. The main types are:
- Acute inflammatory demyelinating polyradiculoneuropathy (AIDP), is the most common form in North America and Europe. The most common sign of AIDP is muscle weakness that starts in the lower part of your body and spreads upward.
- Miller-Fisher syndrome (MFS), in which paralysis starts in the eyes. MFS is also associated with unsteady gait. MFS is less common in the U.S. but more common in Asia.
- Acute motor axonal neuropathy (AMAN) and acute motor-sensory axonal neuropathy (AMSAN) are less common in the U.S. But AMAN and AMSAN are more frequent in China, Japan and Mexico.
When to see a doctor
Call your doctor or health care provider if you have mild tingling in your toes or fingers that doesn’t seem to be spreading or getting worse. Seek emergency medical help if you have any of these severe signs or symptoms:
- Tingling that started in your feet or toes and is now moving up your body
- Tingling or weakness that’s spreading rapidly
- Difficulty catching your breath or shortness of breath when lying flat
- Choking on saliva
Guillain-Barre syndrome is a serious condition that requires immediate hospitalization because it can worsen rapidly. The sooner appropriate treatment is started, the better the chance of a good outcome.
Causes
The exact cause of Guillain-Barre syndrome isn’t known. The disorder usually appears days or weeks after a respiratory or digestive tract infection. Rarely, recent surgery or vaccination can trigger Guillain-Barre syndrome. There have been cases reported following infection with the Zika virus. Guillain-Barre syndrome may occur after infection with the COVID-19 virus. It’s also a rare reaction in those who receive the Johnson & Johnson or AstraZeneca COVID-19 vaccine.
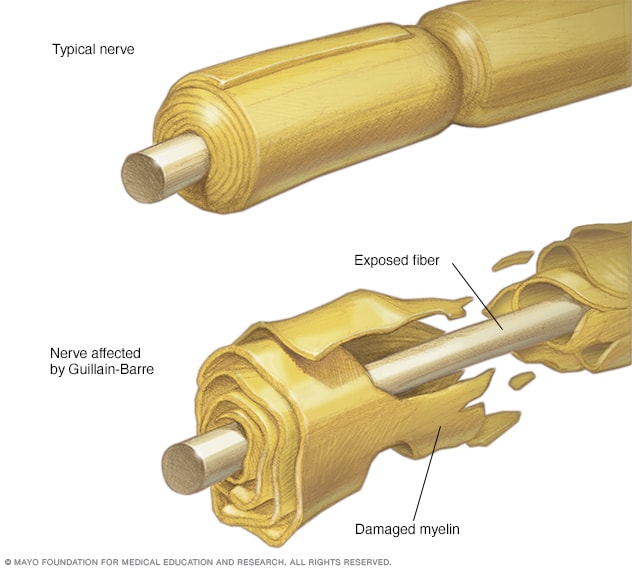
In Guillain-Barre syndrome, your immune system — which usually attacks only invading organisms — begins attacking the nerves. In AIDP, the nerves’ protective covering (myelin sheath) is damaged. The damage prevents nerves from transmitting signals to your brain, causing weakness, numbness or paralysis.
Risk factors
Guillain-Barre syndrome can affect all age groups, but your risk increases as you age. It’s also slightly more common in males than females.
Guillain-Barre syndrome may be triggered by:
- Most commonly, infection with campylobacter, a type of bacteria often found in undercooked poultry
- Influenza virus
- Cytomegalovirus
- Epstein-Barr virus
- Zika virus
- Hepatitis A, B, C and E
- HIV, the virus that causes AIDS
- Mycoplasma pneumonia
- Surgery
- Trauma
- Hodgkin’s lymphoma
- Rarely, influenza vaccinations or childhood vaccinations
- COVID-19 virus
- COVID-19 Johnson & Johnson and AstraZeneca vaccine
Complications
Guillain-Barre syndrome affects your nerves. Because nerves control your movements and body functions, people with Guillain-Barre may experience:
- Breathing difficulties. The weakness or paralysis can spread to the muscles that control your breathing, a potentially fatal complication. Up to 22% of people with Guillain-Barre syndrome need temporary help from a machine to breathe within the first week when they’re hospitalized for treatment.
- Residual numbness or other sensations. Most people with Guillain-Barre syndrome recover completely or have only minor, residual weakness, numbness or tingling.
- Heart and blood pressure problems. Blood pressure fluctuations and irregular heart rhythms (cardiac arrhythmias) are common side effects of Guillain-Barre syndrome.
- Pain. One-third of people with Guillain-Barre syndrome experience severe nerve pain, which may be eased with medication.
- Bowel and bladder function problems. Sluggish bowel function and urine retention may result from Guillain-Barre syndrome.
- Blood clots. People who are immobile due to Guillain-Barre syndrome are at risk of developing blood clots. Until you’re able to walk independently, taking blood thinners and wearing support stockings may be recommended.
- Pressure sores. Being immobile also puts you at risk of developing bedsores (pressure sores). Frequent repositioning may help avoid this problem.
- Relapse. A small percentage of people with Guillain-Barre syndrome have a relapse, experiencing muscle weakness even years after the symptoms ended.
Severe, early symptoms of Guillain-Barre syndrome significantly increase the risk of serious long-term complications. Rarely, death may occur from complications such as respiratory distress syndrome and heart attacks.
TESTS AND PROCEDURES TO RULE OUT NERVE HEALTH.
Electromyography (EMG)
Overview
Electromyography (EMG) is a diagnostic procedure to assess the health of muscles and the nerve cells that control them (motor neurons). EMG results can reveal nerve dysfunction, muscle dysfunction or problems with nerve-to-muscle signal transmission.
Motor neurons transmit electrical signals that cause muscles to contract.
An EMG uses tiny devices called electrodes to translate these signals into graphs, sounds or numerical values that are then interpreted by a specialist.
During a needle EMG, a needle electrode inserted directly into a muscle records the electrical activity in that muscle.
A nerve conduction study, another part of an EMG, uses electrode stickers applied to the skin (surface electrodes) to measure the speed and strength of signals travelling between two or more points.
Why it’s done
Your doctor may order an EMG if you have signs or symptoms that may indicate a nerve or muscle disorder. Such symptoms may include:
- Tingling
- Numbness
- Muscle weakness
- Muscle pain or cramping
- Certain types of limb pain
EMG results are often necessary to help diagnose or rule out several conditions such as:
Muscle disorders, such as muscular dystrophy or polymyositis
Diseases affecting the connection between the nerve and the muscle, such as myasthenia gravis
Disorders of nerves outside the spinal cord (peripheral nerves), such as carpal tunnel syndrome or peripheral neuropathies
Disorders that affect the motor neurons in the brain or spinal cord, such as amyotrophic lateral sclerosis or polio
Disorders that affect the nerve root, such as a herniated disk in the spine
Risks
EMG is a low-risk procedure, and complications are rare. There’s a small risk of bleeding, infection and nerve injury when a needle electrode is inserted.
When muscles along the chest wall are examined with a needle electrode, there’s a minimal risk that it could cause air to leak into the area between the lungs and chest wall, causing a lung to collapse (pneumothorax).
How you prepare
Food and medications
When you schedule your EMG, ask if you need to stop taking any prescription or over-the-counter medications before the exam. If you are taking a medication called Mestinon (pyridostigmine), you should specifically ask if this medication should be discontinued for the examination.
Bathing
Take a shower or bath shortly before your exam to remove oils from your skin. Don’t apply lotions or creams before the exam.
Other precautions
The nervous system specialist (neurologist) conducting the EMG must know if you have certain medical conditions. Tell the neurologist and other EMG lab personnel if you:
Have a pacemaker or any other electrical medical device
Take blood-thinning medications
Have haemophilia, a blood-clotting disorder that causes prolonged bleeding
What you can expect
Before the procedure.
You’ll likely be asked to change into a hospital gown for the procedure and lie down on an examination table. To prepare for the study, the neurologist or a technician places surface electrodes at various locations on your skin depending on where you’re experiencing symptoms. Or the neurologist may insert needle electrodes at different sites depending on your symptoms.
During the procedure
When the study is underway, the surface electrodes will at times transmit a tiny electrical current that you may feel as a twinge or spasm. The needle electrode may cause discomfort or pain that usually ends shortly after the needle is removed.
During the needle EMG, the neurologist will assess whether there is any spontaneous electrical activity when the muscle is at rest—activity that isn’t present in healthy muscle tissue — and the degree of activity when you slightly contract the muscle.
He or she will give you instructions on resting and contracting a muscle at appropriate times. Depending on what muscles and nerves the neurologist is examining, he or she may ask you to change positions during the exam.
If you’re concerned about discomfort or pain at any time during the exam, you may want to talk to the neurologist about taking a short break.
After the procedure
You may experience some temporary, minor bruising where the needle electrode was inserted into your muscle. This bruising should fade within several days. If it persists, contact your primary care doctor.
Results
The neurologist will interpret the results of your exam and prepare a report. Your primary care doctor, or the doctor who ordered the EMG, will discuss the report with you at a follow-up appointment.
LUMBER PUCTURE / SPINAL TAP
Overview
 Lumbar puncture (spinal tap)Enlarge image
Lumbar puncture (spinal tap)Enlarge image
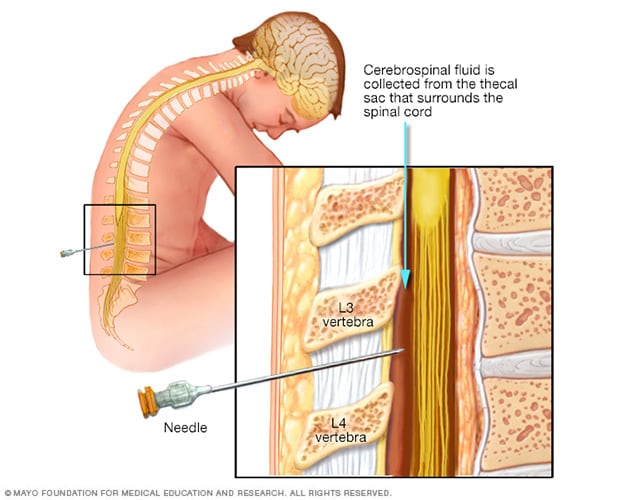
A lumbar puncture (spinal tap) is a test used to diagnose certain health conditions. It’s performed in your lower back, in the lumbar region. During a lumbar puncture, a needle is inserted into the space between two lumbar bones (vertebrae) to remove a sample of cerebrospinal fluid. This is the fluid that surrounds your brain and spinal cord to protect them from injury.
A lumbar puncture can help diagnose serious infections, such as meningitis; other disorders of the central nervous system, such as Guillain-Barre syndrome and multiple sclerosis; bleeding; or cancers of the brain or spinal cord. Sometimes a lumbar puncture is used to inject anesthetic medications or chemotherapy drugs into the cerebrospinal fluid.
Why it’s done
A lumbar puncture (spinal tap) may be done to:
- Collect cerebrospinal fluid to check for infections, inflammation or other diseases
- Measure the pressure of cerebrospinal fluid
- Inject spinal anesthetics, chemotherapy drugs or other medications
- Inject dye (myelography) or radioactive substances (cisternography) into cerebrospinal fluid to make diagnostic images of the fluid’s flow
Information gathered from a lumbar puncture can help diagnose:
Serious bacterial, fungal and viral infections, including meningitis, encephalitis and syphilis
Bleeding around the brain (subarachnoid hemorrhage)
Certain cancers involving the brain or spinal cord
Certain inflammatory conditions of the nervous system, such as multiple sclerosis and Guillain-Barre syndrome
Autoimmune neurological conditions
Alzheimer’s disease and other forms of dementia
Risks
Although lumbar puncture (spinal tap) is generally recognized as safe, it does carry some risks. These include:
Post-lumbar puncture headache. As many as 25% of people who undergo a lumbar puncture develop a headache afterward due to fluid leaking into nearby tissues.The headache typically starts several hours up to two days after the procedure and may be accompanied by nausea, vomiting and dizziness. The headaches are usually present when sitting or standing and resolve after lying down. Post-lumbar puncture headaches can last from a few hours to a week or more.
Back discomfort or pain. You may feel pain or tenderness in your lower back after the procedure. The pain might radiate down the back of your legs.
Bleeding. Bleeding may occur near the puncture site or, rarely, in the epidural space.
Brainstem herniation. Increased pressure within the skull due to a brain tumor or other space-occupying lesion can lead to compression of the brainstem after a sample of cerebrospinal fluid is removed. To prevent this rare complication, a computerized tomography (CT) scan or magnetic resonance imaging (MRI) scan is often performed before a lumbar puncture to look for any sign of a space-occupying lesion resulting in increased intracranial pressure. A detailed neurological examination can also help rule out a significant space-occupying lesion.
How you prepare
Before your lumbar puncture (spinal tap), your health care provider takes your medical history, does a physical exam, and orders blood tests to check for bleeding or clotting disorders. Your provider may also recommend a CT scan or MRI to determine if you have any abnormal swelling in or around your brain.
Food and medications
Your health care provider will give you specific instructions about food, drink and medications.
Tell your provider if you’re taking blood-thinning or other anticoagulant medications. Examples include warfarin (Jantoven), clopidogrel (Plavix) and apixaban (Eliquis). Also, tell your provider if you’re allergic to any medications, such as numbing medications (local anesthetics).
What you can expect
A lumbar puncture (spinal tap) is usually done in an outpatient facility or a hospital. Your health care provider will talk to you about the potential risks, and any discomfort you might feel during the procedure.
If a child is having a lumbar puncture, a parent may be allowed to stay in the room in some cases. Talk to your child’s health care provider about whether this will be possible.
Before the procedure
You may be asked to change into a hospital gown, although in some cases you may have the procedure while wearing your own clothing. There are a few possible positions for a lumbar puncture (spinal tap). Usually, you lie on your side with your knees drawn up to your chest, or you sit and lean forward on a stable surface. These positions flex your back, widening the spaces between your vertebrae and making it easier for your healthcare provider to insert the needle. Your back is washed with antiseptic soap or iodine and covered with a sterile sheet.
For an infant or a young child, someone will hold the child in position during the procedure.
During the procedure
A local anaesthetic is injected into your lower back to numb the puncture site before the needle is inserted. The local anaesthetic will sting briefly as it’s injected.
A thin, hollow needle is inserted between the two lower vertebrae (lumbar region), through the spinal membrane (dura) and into the spinal canal. You may feel pressure in your back during this part of the procedure.
Once the needle is in place, you may be asked to change your position slightly.
The cerebrospinal fluid pressure is measured, a small amount of fluid is withdrawn and the pressure is measured again.
The needle is removed, and the puncture site is covered with a bandage.
The procedure usually lasts about 45 minutes. Your healthcare provider may suggest lying down after the procedure.
Sometimes, an ultrasound may be used as a guide during a lumbar puncture in infants and young children. The ultrasound can help prevent inserting the needle too far.
After the procedure
Plan to rest. Don’t participate in strenuous activities on the day of your lumbar puncture (spinal tap). You may return to work if your job doesn’t require you to be physically active. Discuss your activities with your healthcare provider if you have questions.
Take a pain medication. A nonprescription pain-relieving medication that contains acetaminophen (Tylenol, others) can help reduce a headache or back pain. If your headache becomes severe, call your healthcare provider.
Results
The spinal fluid samples from the lumbar puncture (spinal tap) are sent to a laboratory for analysis. Lab technicians check for several things when examining spinal fluid, including:
General appearance. Spinal fluid is normally clear and colourless. If the colour is orange, yellow or pink, it might indicate abnormal bleeding. Spinal fluid that is green might indicate an infection or the presence of bilirubin.
Protein (total protein and the presence of certain proteins). Elevated levels of total protein — greater than 45 milligrams per deciliter (mg/dL) — may indicate an infection or another inflammatory condition. Specific lab values may vary from medical facility to medical facility.
White blood cells. Spinal fluid normally contains up to five white blood cells per microliter. Increased numbers may indicate an infection or other condition. Specific lab values may vary from medical facility to medical facility.
Sugar (glucose). A low glucose level in spinal fluid may indicate an infection, tumor or another condition.
Microorganisms. The presence of bacteria, viruses, fungi or other microorganisms can indicate an infection.
Cancer cells. The presence of abnormal cells in spinal fluid — such as tumor or immature blood cells — can indicate certain types of cancer.
Lab results are combined with information obtained during the test, such as spinal fluid pressure, to help make a possible diagnosis.
Your healthcare provider generally gives you the results within a few days, but it could take longer. Ask when you can expect to receive the results of your test.
Write down questions that you want to ask your healthcare provider. Don’t hesitate to ask other questions that may come up during your visit. Questions you may want to ask include:
Based on the results, what are my next steps?
What kind of follow-up, if any, should I expect?
Are there any factors that might have affected the results of this test and, therefore, may have altered the results?
Will I need to repeat the test at some point?
Usually I do not read article on blogs however I would like to say that this writeup very compelled me to take a look at and do it Your writing style has been amazed me Thank you very nice article
I do trust all the ideas youve presented in your post They are really convincing and will definitely work Nonetheless the posts are too short for newbies May just you please lengthen them a bit from next time Thank you for the post